
Biceps Tendonitis

Anatomy, Symptoms, and Treatment Options for Biceps Tendonitis
The biceps muscle has two tendons that attach to the shoulder. The short head tendon attaches to the coracoid, the small bony bump on the front of the shoulder. The other, the long head tendon, goes through an opening in the rotator cuff between two tendons and attaches to the top of the glenoid (socket of the shoulder). This is a long, rope-like tendon that is commonly inflamed.
Biceps tendonitis causes pain over the front of the shoulder. Common symptoms include pain putting on a bra, reaching into the back seat of a car, or putting on a jacket. The pain can be bothersome at night as well. Biceps tendonitis is commonly associated with other diagnoses such as rotator cuff tendonitis or tears, shoulder arthritis, and labral tears.
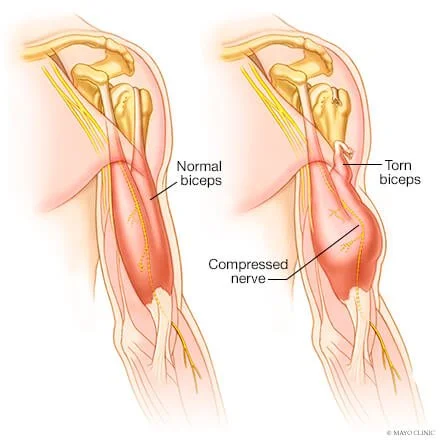
The anatomy of the long head of the biceps tendon predisposes it to wear and tear. Chronic inflammation and repetitive overhead sports and lifting can cause cumulative damage to the tendon. Occasionally the damage is so severe that the tendon tears completely. This creates an asymmetry in the contour of the biceps and is called a “Popeye Deformity.” Since there is another attachment of the biceps muscle at the shoulder (the short head), most of the time, long head of the biceps ruptures do not require surgery.

Non-Surgical Treatment
-
Avoid activities that re-create the sharp pain as best as possible. Limit repetitive reaching or lifting.
-
Physical therapy is important to strengthen and rebalance the muscles of your shoulder. PT helps decrease pain and inflammation in the shoulder.
-
NSAIDS such as ibuprofen or naproxen can help with swelling and pain.
-
Ultrasound-guided injections of corticosteroids around the biceps tendon can provide improvement in pain and inflammation.
Surgical
Treatment
When pain persists despite a course of nonsurgical management, surgery is an option. Surgery for biceps tendonitis involves removing the diseased tendon and re-attaching the healthy portion of the biceps tendon to the humerus. This can be done arthroscopically through small incisions around the shoulder or a small 2-3 cm open incision on the front of the shoulder. Dr. Walcott will discuss the pros and cons of each option with you to determine your preferred approach.